
TL;DR:
- End of life care focuses on providing comfort and dignity for individuals in their final weeks or months, with support from interdisciplinary teams. It includes symptom management, emotional support, spiritual care, and practical planning, emphasizing early conversations and legal directives to reduce family distress. Hospice care, a form of end of life support, is reversible and designed to prioritize quality over curative treatments, often delivered at home.
End of life care is the comprehensive medical, emotional, and practical support provided to individuals nearing the end of their life, with the focus placed firmly on comfort and dignity rather than cure. It is the recognised term used by the NHS, hospice organisations, and palliative care teams across the UK to describe this period of care. For families and caregivers, understanding what this care involves, who provides it, and how to plan for it can make an enormous difference to the experience of everyone involved. This guide explains end of life care clearly, covering the types of support available, how to make informed decisions, and how to be present for your loved one in the most meaningful way.
What does end of life care mean, and how does it differ from palliative care?
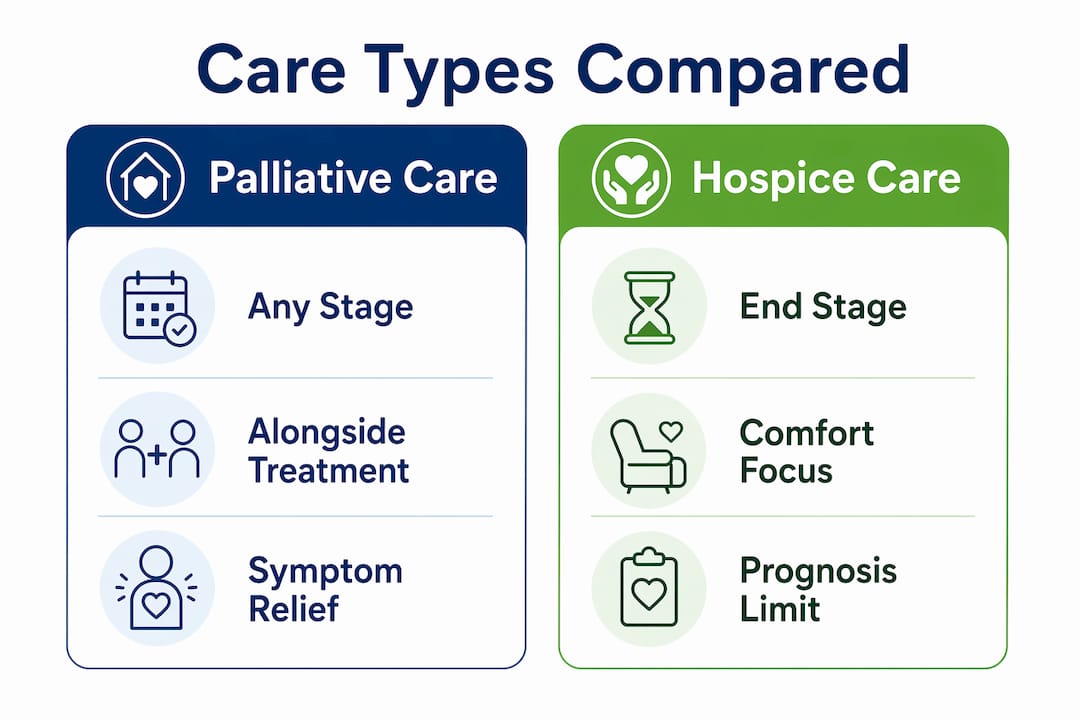
End of life care and palliative care are closely related but not identical. Palliative care is specialist support that can begin at any stage of a serious illness, running alongside curative treatments to manage symptoms and improve quality of life. End of life care is the phase that follows when the focus shifts entirely away from cure and towards comfort in the final weeks, months, or days of life.
Hospice care sits within this end of life phase. Hospice care is typically intended for individuals with a prognosis of six months or less, and it requires the cessation of curative treatments. Palliative care, by contrast, can be provided at any stage of a serious illness alongside active treatment. This distinction matters because families sometimes delay accessing hospice support out of fear that it signals giving up. It does not.
| Feature | Palliative care | Hospice care |
|---|---|---|
| When it begins | Any stage of serious illness | Prognosis of six months or less |
| Curative treatment | Continues alongside care | Ceases on entry |
| Primary goal | Symptom relief and quality of life | Comfort, dignity, and peaceful death |
| Setting | Hospital, home, or clinic | Home, hospice unit, or care home |
| Bereavement support | Variable | Included for up to 13 months post-death |
One important reassurance for families is that hospice care can be revoked at any time if a patient wishes to resume curative treatment. Hospice is not an irreversible decision, and eligibility is renewable beyond the initial six months if criteria remain met.
Pro Tip: If your loved one is receiving palliative care and their condition is declining, ask their care team directly whether a referral to hospice services would be appropriate. Many families access hospice support later than they could have, missing weeks of additional comfort care.
What practical support does end of life care provide?
End of life care is delivered by interdisciplinary teams that include nurses, doctors, social workers, chaplains, and trained volunteers. Hospice programmes include bereavement support services such as grief counselling, memorial events, and family check-in calls, often continuing for up to 13 months after the patient’s death, with 24/7 phone availability for urgent needs.
The practical support provided covers a wide range of needs:
- Symptom management: Pain relief, breathlessness control, nausea management, and skin care to keep your loved one as comfortable as possible.
- Emotional and psychological support: Counselling for both the patient and family members, addressing fear, grief, and anxiety at every stage.
- Spiritual care: Chaplaincy services that respect all faiths and none, helping patients and families find meaning and peace.
- Family education: Guidance on what to expect physically and emotionally, so you feel prepared rather than frightened.
- Respite care: Short-term relief for family caregivers who need rest without compromising the quality of their loved one’s care.
- Bereavement services: Structured grief support that continues after death, recognising that the family’s needs do not end when the patient dies.
Over 80% of hospice care in many regions is delivered in the patient’s home. This means that for most families, end of life care is not something that happens in a hospital ward. It happens in familiar surroundings, with professional support coming to you. Knowing this helps families plan more confidently for what lies ahead.
How can families make informed end of life care decisions?

The most effective end of life care decisions begin with conversations that happen well before a crisis. Early conversations about end-of-life values and preferences are the single most reliable way to reduce family stress and honour patient wishes when the time comes. These discussions do not need to be frightening. They are an act of care.
Here are the steps families and caregivers can take to plan well:
- Start the conversation early. Ask your loved one about their values, fears, and wishes while they are still able to express them clearly. What matters most to them? Where do they want to be cared for?
- Create an advance directive. This legal document records your loved one’s wishes regarding treatments such as mechanical ventilation, resuscitation, and hospitalisation. Advance care planning must cover more than a Do Not Resuscitate order.
- Appoint a healthcare proxy. This is a trusted person who can make medical decisions on behalf of your loved one if they lose capacity. Choose someone who understands their values, not just their wishes.
- Discuss quality of life goals with the care team. Ask the medical team to explain the likely trade-offs between treatments and comfort. What does each option mean for daily life and dignity?
- Recognise when to transition from curative to comfort care. The transition from palliative to hospice care is gradual, based on clinical judgement when curative treatments cease to be effective.
- Prepare a clear emergency plan. Know who to call when symptoms worsen at home. Calling emergency services during a home death often results in unwanted aggressive interventions. Your hospice or palliative care team is the right first call.
Pro Tip: Write down your loved one’s care team contacts, medication list, and advance directive location in a single document kept somewhere visible at home. In a moment of distress, having this information immediately to hand prevents panic and poor decisions.
You can also find practical guidance on palliative care at home to help you understand what to expect when care is delivered in a home setting.
What legal and ethical end of life options exist beyond standard care?
Beyond palliative and hospice care, some families explore less commonly discussed but legally available choices. Understanding these options helps you support your loved one’s autonomy with confidence.
- Medical Aid in Dying (MAiD): MAiD is legal in 10 US states with conditions including a terminal prognosis and confirmed mental competence. It allows a patient to request a prescription to hasten death. In the UK, assisted dying is not currently legal, though this remains an active area of public and parliamentary debate.
- Voluntary stopping of eating and drinking (VSED): VSED is accessible without a terminal diagnosis and involves a patient choosing to stop all oral intake. It is managed with palliative care for symptom relief over a period of one to two weeks. It is considered a compassionate choice when a patient has decision-making capacity and a clear wish to hasten a natural death.
- Withdrawal of life-sustaining treatment: Patients or their proxies can legally request the withdrawal of treatments such as ventilation or artificial nutrition. This is a recognised and ethical choice, not a form of abandonment.
The emotional impact of these decisions on families can be profound. Seeking support from a social worker, counsellor, or chaplain during this process is not a sign of weakness. It is good care for yourself as well as your loved one. Respecting patient autonomy means supporting their choices even when those choices are difficult to witness.
What physical signs should caregivers expect in the final days?
Recognising the physical changes that occur near death helps caregivers respond with calm and compassion rather than alarm. Physical signs such as irregular breathing, decreased consciousness, mottled skin, and noisy breathing commonly occur in the final hours and days. These are normal parts of the dying process.
Key things to know and do during this time:
- Noisy breathing (the “death rattle”) is caused by secretions in the throat. It does not distress the patient, though it can be distressing to hear. Repositioning and medication can reduce it. Contact the care team rather than attempting to manage it alone.
- Decreased consciousness means your loved one may not respond to speech or touch. Continue to speak gently and calmly. Hearing is believed to persist even when other responses have faded.
- Mottled or discoloured skin on the hands, feet, and knees indicates reduced circulation. Keep your loved one warm and comfortable.
- Irregular or Cheyne-Stokes breathing involves long pauses between breaths. This is normal and does not cause suffering.
- Reduced eating and drinking is the body’s natural response to shutting down. Do not try to force food or fluids. Small amounts of mouth care keep lips moist and comfortable.
Providing a calm presence and consistent symptom management offers the most meaningful support during this time. You do not need to do more. Being there, speaking softly, and holding a hand is often the most important thing a caregiver can do. Guidance on promoting dignity in care can help you maintain your loved one’s sense of self and respect throughout.
Key takeaways
End of life care is most effective when families understand their options early, communicate clearly, and access professional support before a crisis occurs.
| Point | Details |
|---|---|
| Palliative vs hospice care | Palliative care runs alongside treatment; hospice begins when curative care ends and prognosis is six months or less. |
| Hospice is reversible | Patients can leave hospice at any time to resume curative treatment, so it is not a final or irreversible decision. |
| Plan before a crisis | Advance directives, healthcare proxies, and written emergency plans prevent distressing and unwanted interventions. |
| Physical signs are normal | Noisy breathing, mottled skin, and reduced consciousness are expected near death and do not indicate suffering. |
| Presence is powerful | Calm companionship and symptom management are the most meaningful forms of support in the final days. |
What I have learned from supporting families through end of life care
One thing stands out after years of working alongside families in this situation: the families who feel most at peace are almost always the ones who had the conversation early. Not because it was easy, but because they did it anyway.
Many caregivers arrive at end of life care carrying a misconception that asking about hospice means they have stopped fighting for their loved one. The opposite is true. Choosing comfort care is an act of profound love. It says: I want your remaining time to be as good as it can possibly be.
The other thing I have seen repeatedly is that families underestimate the value of simply being present. When there is nothing more to treat, there is still everything to give. A familiar voice, a hand held, a favourite piece of music playing quietly. These things matter more than most people realise.
If you are a caregiver reading this, please do not wait until you are in crisis to seek information or support. The more you understand now, the more confident and present you will be when it matters most. You deserve support too, not just your loved one.
— Dan
How Kells-care supports families with end of life care at home
Kells-care has been providing high-quality domiciliary care across London for over 30 years, and we understand how much it means to families to have their loved one cared for at home with dignity and compassion. Our fully qualified, DBS-checked carers can provide personalised support that complements palliative and end of life care, from regular check-in visits to round-the-clock assistance. We are regulated by the Care Quality Commission (CQC) and tailor every care plan to the individual. Download our free home care guide to understand your options, or explore our home care services to find the right level of support for your family. We are here to help.
FAQ
What is end of life care?
End of life care is specialist support focused on comfort, dignity, and quality of life for individuals in the final stage of a serious illness. It includes medical symptom management, emotional support, spiritual care, and practical assistance for both patients and their families.
How long does end of life care last?
End of life care can last from a few days to several months, depending on the individual’s condition. Hospice care specifically applies when a prognosis of six months or less has been given, though this timeline is flexible and care continues as long as it is needed.
Is hospice care the same as giving up?
Hospice care is not giving up. It is a deliberate choice to prioritise comfort and quality of life over curative treatment. Patients can also leave hospice at any time to resume active treatment if they choose.
What should I do if my loved one’s condition worsens suddenly at home?
Contact your hospice or palliative care team immediately rather than calling emergency services. Pre-arranged plans with your care team allow symptoms to be managed at home, avoiding unwanted hospital admissions and preserving the quality of your loved one’s experience.
What is an advance directive and why does it matter?
An advance directive is a legal document that records a person’s wishes regarding medical treatment if they lose the ability to communicate. It covers decisions such as resuscitation, ventilation, and hospitalisation, and helps the care team and family honour the patient’s values during end of life care.


